Education-Based
Evaluations for
Autism Spectrum Disorder
September 9, 2015 www.michigan.gov/autism

Table of Contents
Acknowledgments ................................................................................................................. 3
Purpose ................................................................................................................................. 3
Introduction .......................................................................................................................... 4
Michigan Administrative Rules for Special Education (MARSE) ASD Eligibility Criteria ............. 5
MARSE Eligibility Criteria.......................................................................................................................... 5
Qualitative Impairments in Reciprocal Social Interactions ................................................................... 6
Qualitative Impairments in Communication ......................................................................................... 8
Restricted, Repetitive, and Stereotyped Behaviors ............................................................................. 10
Unusual or Inconsistent Response to Sensory Stimuli ......................................................................... 12
Age ...................................................................................................................................................... 12
Adverse Impact....................................................................................................................................... 12
Academic ............................................................................................................................................. 13
Behavioral ........................................................................................................................................... 13
Social ................................................................................................................................................... 13
Need for Special Education Programs and/or Related Services ............................................................. 14
Education-based Evaluation for ASD .................................................................................... 14
Review of Existing Evaluation Data (REED) ............................................................................................ 16
Completion of Evaluation Components .................................................................................................. 16
Results Review Meeting ......................................................................................................................... 21
Multidisciplinary Evaluation Team Report ............................................................................................. 22
Individualized Education Program ......................................................................................................... 23
Differential Eligibility Decision-Making ................................................................................ 23
Considerations for Evaluation of Young Children .................................................................. 25
Appendices ......................................................................................................................... 28
References .......................................................................................................................... 44
The Michigan Autism Council 2 www.michigan.gov/autism
Acknowledgments
Writing/Drafting Team
Autism Council Education Subcommittee Evaluation Workgroup
Dorie France, Rob Dietzel, Joanne Winkelman, Stephanie Dyer, and Kelly Dunlap
Lead Editors
Stephanie Dyer and Kelly Dunlap
Reviewers
Deb Koepke, Pamela Lemerand, Valerie Mierzwa, Leigh McFarland, and Lindsey Harr-Smith
Significant Contributions
Clinton County Regional Educational Service Agency (RESA) Evaluation Process, Charlevoix–
Emmet Intermediate School District (ISD) Autism Spectrum Disorder Eligibility Guidelines,
and Centralized Evaluation Team Process (Dave Schoemer and Maureen Ziegler)
Purpose
The Michigan Autism Spectrum Disorder (ASD) State Plan recommends that education-
based multidisciplinary evaluation teams have access to information and training in ASD
eligibility determination to improve the consistency of practices. The purpose of this
document is to provide guidance to schools to develop evaluation processes to ensure
accurate eligibility decisions, improve cross-agency collaboration to reduce duplication,
ensure a seamless process for families, and provide relevant information to inform the
Individualized Education Program (IEP). In some instances, this document addresses
considerations of evaluation components that exceed requirements of federal law
or Michigan Administrative Rules for Special Education (MARSE).
The Michigan Autism Council 3 www.michigan.gov/autism
Introduction
The purpose of an education-based evaluation is to determine a student’s eligibility for
special education programs or services under the MARSE criteria, not to provide a clinical
diagnosis. However, according to the Michigan ASD State Plan survey (2012), there is often
confusion between a clinical diagnosis of ASD and ASD special education eligibility criteria.
The confusion is further exacerbated when a child receives a clinical diagnosis of ASD but
then does not meet the education-based eligibility criteria under ASD. As such, it is
important to outline the differences in process and purpose of evaluations between the two
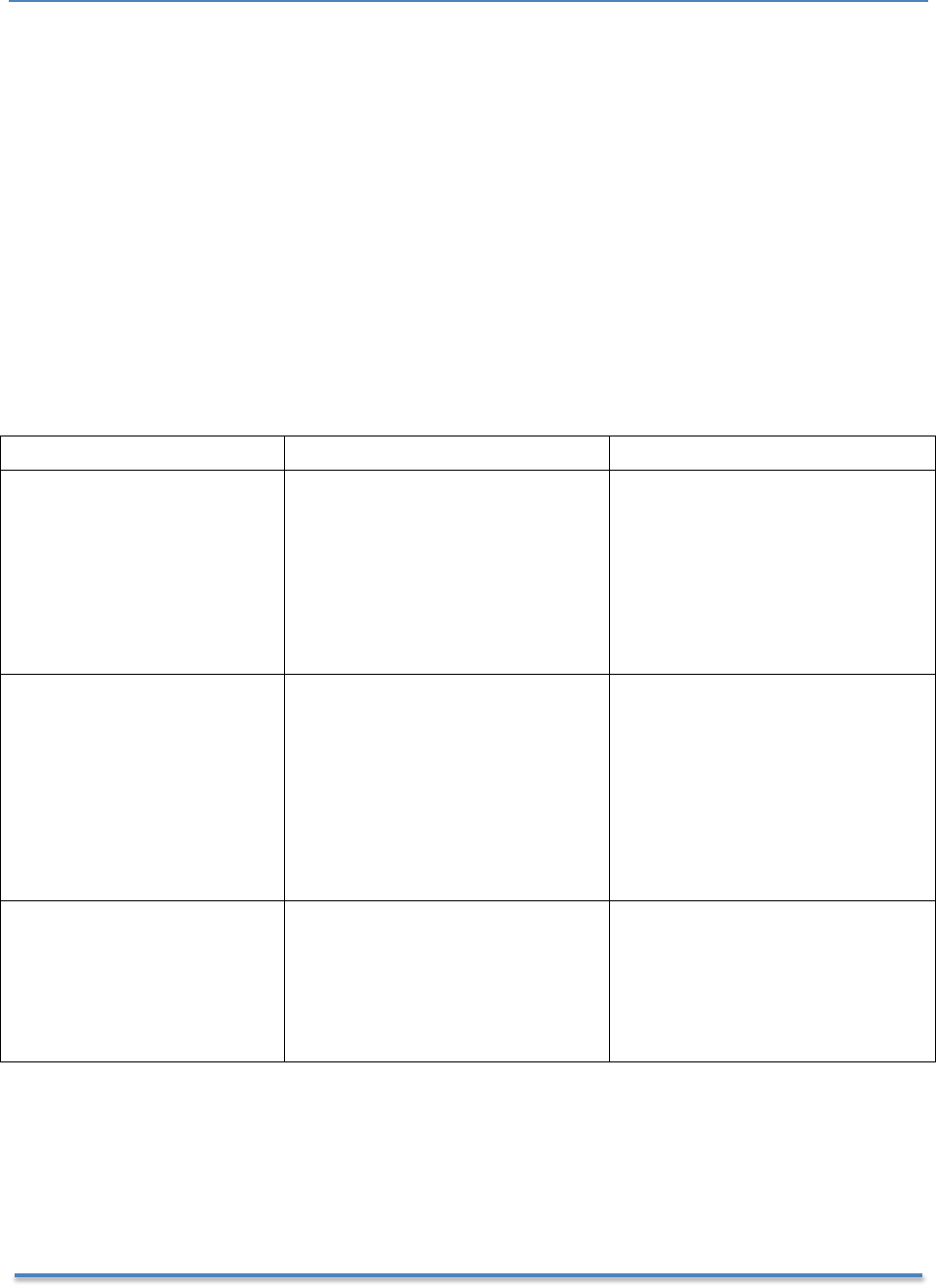
to enhance understanding across school personnel, clinical staff, and families. Below is a
brief comparison of the various components of evaluation across the school and clinical
models:
Education-Based Eligibility
Clinical/Medical Diagnosis
Purpose/
Function
• Determine special education
eligibility or ineligibility
• Determine educational impact
• Determine need for specially
designed instruction
• Inform IEP and special
education services
• Make Clinical/Medical/
Behavioral Health Diagnosis
• Determine insurance or Medicaid
Autism benefit eligibility
• Access non-educational agency
services
• Dictate medical/clinical treatment
Criteria/Tools
to Make
Determination
• MARSE ASD criteria
• Use of tools individually
determined based on what
questions need to be
answered
• Diagnostic and Statistical Manual
for Mental Disorders Fifth Edition
(DSM-5)
• Clinical diagnostic assessment
tools (e.g. Autism Diagnostic
Observation Schedule (ADOS))
• For additional information, see
Medical Services Administration
(MSA) Bulletin 13-09
Team
Members
• Multidisciplinary team
including a psychologist/
psychiatrist, authorized
provider of speech and
language services, and school
social worker are required
• Practitioners can make
independent diagnostic decisions
Plan for
Evaluation*
• Review Existing Evaluation
Data (REED)
• No evaluation plan requirement
Observations**
• Multiple observations in
varied environments over
time
• Generally includes observations in
an office or clinic setting
*Not required for initial evaluations, but recommended
**Not required, but considered a necessary component
Because the process and purpose for evaluations are different, a clinical diagnosis of ASD is
not required or sufficient for the determination of special education eligibility. If clinical
diagnostic information is available, it must be considered in the evaluation process, but the
The Michigan Autism Council 4 www.michigan.gov/autism
final determination of eligibility may still require additional education-based assessments or
observations.
Further, given these differences in tools and processes, it is not uncommon for
disagreements in ASD eligibility and diagnosis to occur. As such, it is important for
education-based multidisciplinary evaluation teams and clinical evaluators to work
collaboratively to assist families in understanding these differences and the reasons the
differences exist. Information on effective collaboration can be found in the Michigan Autism
Council’s Collaboration Matrix (2014).
In recent years, progress has been made in both the clinical and educational fields in the
assessment and identification of ASD. This document outlines the core components of
eligibility determination for ASD.
Michigan Administrative Rules for Special
Education (MARSE) ASD Eligibility Criteria
As it is with all eligibility areas, special education eligibility for ASD is a three-pronged
process:
1. The student must meet the MARSE eligibility criteria for ASD,
2. The ASD must adversely affect the student’s educational performance in
academic, behavioral, or social domains, and
3. The impact must require and necessitate special education programs and/or
services.
A multidisciplinary evaluation team is required to provide evidence in all three areas to
determine a student eligible for special education programs and/or services. Below is
information to assist the multidisciplinary evaluation team in gathering relevant data to
address all three required areas of eligibility.
MARSE Eligibility Criteria
To meet the MARSE eligibility criteria for ASD, a student must demonstrate characteristics in
all three of the following domains:
1. Qualitative impairments in reciprocal social interactions,
2. Qualitative impairments in communication, and
3. A restricted range of interests or repetitive behavior.
Two additional factors may be considered in determining eligibility under the ASD criteria:
4. Unusual or inconsistent response to stimuli
5. Age
The Michigan Autism Council 5 www.michigan.gov/autism

The complete the MARSE eligibility criteria (R 340.1715) are found in Appendix A. However,
a review of the three domains with example behavioral characteristics is provided below:
Qualitative Impairments in Reciprocal Social Interactions
A qualitative impairment is defined as atypical or considerably different from other students
the same age. According to MARSE, a qualitative impairment in reciprocal social interactions
would include at least two of the following four characteristics:
1. Marked impairment in the use of multiple nonverbal behaviors, such as eye-to-
eye gaze, facial expression, body postures, and gestures, to regulate social
interaction.
Marked impairment in this area means substantial and sustained difficulty using
nonverbal behaviors to augment communication for the purposes of the social partner.
This criterion is not intended to define the presence or absence of nonverbal behavior
but rather the use of nonverbal behavior to regulate social communication, particularly
where words fail.
Marked impairment also implies that the difficulties are clearly evident and observed
across multiple environments and people over time. Evidence of marked impairment in
nonverbal behaviors may include, but is not limited to, the following:
• Differences in eye-to-eye gaze (e.g. seems to look “through” a person, limited or no
eye contact or eye gaze to initiate, sustain, or guide social interaction, has fleeting or
inconsistent eye contact)
• Differences in facial expression (e.g. lacks emotion or appropriate facial affect for the
social situation, lacks accurate facial expression to reflect internal feelings, facial
expressions seem rehearsed or mechanical, limited or no use of facial expression to
guide communication)
• Differences in body posture (e.g. difficulty maintaining appropriate body space,
awkward/stiff response or movement, gait challenges)
• Differences in spontaneous use of gestures (e.g. lacks understanding of the use of
nonverbal cues (e.g. pointing, head nod, waving), does not respond to
communication partner signals to start or end a conversation)
2. Failure to develop peer relationships appropriate to developmental level.
Students may fail to develop appropriate peer relationships for a variety of reasons. For
students with ASD, failure to develop reciprocal relationships with peers results from
deficits in social reciprocity (i.e. the give and take in social interaction) and the inability
to understand the perspectives of others.
In addition, the quality of peer relationships must be made in comparison to peers at the
same age and developmental level. Evidence of failure to develop reciprocal peer
relationships may include, but is not limited to, the following:
The Michigan Autism Council 6 www.michigan.gov/autism

• Lack of understanding of age-appropriate humor and jokes
• Disruption of ongoing activities when entering play or social circles; may insist on
controlling the play when engaging with others
• Lack of initiation or sustained interactions with others
• Preference to play alone
• Continuous failure in trying to understand social nuances and follow social rules
• Desire for friendships but has multiple failed attempts
• Misinterpretation of social cues or communication intent of others
• Tolerance of peers but no spontaneous engagement in conversation or activity
• Confusion with the telling of lies
• Policing peers (e.g. reporting rule infractions on the playground)
3. Marked impairment in spontaneous seeking to share enjoyment, interests, or
achievements with other people (e.g. a lack of showing, bringing, or pointing
out objects of interest).
Marked impairment in this area means substantial lack of spontaneous (i.e. without
prompting) sharing and showing, often referred to as joint attention. According to Oates
& Grayson (2004), joint attention is defined as the shared focus or experience of two or
more individuals on an object or activity. This typically begins to develop around two
months of age with dyadic (i.e. two persons) exchanges using looks, noises, and mouth
movements. Lack of sharing with others also results from deficits in understanding the
perspectives of others.
Marked impairment in this area must be clearly evident across multiple people and
environments over time. Evidence of impairment in spontaneous seeking to share may
include, but is not limited to, the following:
• Deficits in the use of pointing to orient another to an object or event
• Limited number of attempts to share achievements or items of interest with others
as compared to peers
• Bringing objects or items to others for the purposes of getting needs met, but not for
a shared experience
• Lack of response to others sharing enjoyment, interests, or achievements (e.g.
shifting conversations to one’s own interest rather than responding to the interests
of others)
4. Marked impairment in the areas of social or emotional reciprocity.
Reciprocity is defined as the mutual give and take of social interactions. Marked
impairment in this area implies significant difficulty recognizing and responding to the
needs, intentions, perspectives, and feelings of others across multiple environments and
people over time. Evidence of impairment in social or emotional reciprocity may include,
but is not limited to, the following:
• Limited to no use of social smiling; rarely offers spontaneous social smiles
• Lack of interest in the ideas of others
The Michigan Autism Council 7 www.michigan.gov/autism

• Aloofness and indifference toward others
• Seemingly rude statements to others without filter or negative intent (e.g. telling
someone to stop eating chips because they are fat, as if they are doing that person a
favor)
• Difficulty explaining their own behaviors in context of impact on others
• Difficulty predicting how others feel or think
• Problems inferring the intentions or feelings of others
• Failure to understand how their behavior impacts how others think or feel
• Problems with social conventions (e.g. turn-taking, politeness, and social space)
• Lack of appropriate response to someone else’s pain or distress (e.g. laughing when
others are upset)
• Creating arbitrary social rules to make sense of ambiguous social norms (e.g. “All
people fall into one of three categories: jocks, friends, or people who make bad
decisions.”)
Qualitative Impairments in Communication
A qualitative impairment is defined as atypical development or considerable differences as
compared to other students the same age. According to MARSE, qualitative impairments in
communication include at least one of the following:
1. Delay in or total lack of the development of spoken language not accompanied
by an attempt to compensate through alternative modes of communication
such as gesture or mime.
Typical development of language includes babbling by 12 months, single word use by 16
months, and two-word phrases by 24 months of age. Some children fail to develop
language yet compensate by using alternative communication modes such as gestures,
facial expressions, and other nonverbal behaviors.
Some children with ASD, however, do not seem to recognize that words have a
communicative intent. As such, they fail to compensate for their lack of language
development, although they may ensure their needs get met (e.g. using an adult as a
tool to get a snack or toy or shoving someone to get them out of the way).
In some instances, children with ASD may begin to develop spoken language and then
lose the language they have acquired. Evidence of delay in or lack of the development of
spoken language not accompanied by attempts to compensate may include, but is not
limited to, the following:
• Pulling an adult to a particular area to get a snack or toy
• Standing or screaming near the refrigerator in the absence of an adult
• Use of words not directed at others (e.g. gibberish, mumbling)
• Challenging behavior in lieu of alternate communication (e.g. hitting, biting, pushing,
screaming)
The Michigan Autism Council 8 www.michigan.gov/autism

2. Marked impairment in pragmatics or in the ability to initiate, sustain, or engage
in reciprocal conversation with others.
“Pragmatics” is a term used to explain the give and take of social language. Deficits in
pragmatics for students with ASD result from deficits in understanding the perspectives
of others and lack of social reciprocity.
Marked impairment implies that difficulty with pragmatics is clearly evident in multiple
environments and people across time. Evidence of marked impairment in pragmatics
may include, but is not limited to, the following:
• Difficulty with the social aspects of language (e.g. understanding non-literal language
used in conversation)
• Issues with prosody (e.g. flat and emotionless or high and pitchy with atypical
rhythm or rate)
• Difficulty changing language according to the needs of the listener (e.g. not giving
background information to an unfamiliar listener or not speaking differently in a
classroom than on a playground)
• Difficulty initiating, sustaining, or ending conversations with others
• Difficulty using repair strategies when communication breaks down
• Difficulty following the rules of conversations and storytelling (e.g. taking turns in
conversation, staying on topic, rephrasing when misunderstood, proximity, use of
eye contact)
• Talking for extended periods of time about a subject of the student’s liking,
regardless of the listener’s interest
• Talking at someone in a monologue rather than conversing
• Interpreting what others say according to the most basic or literal meaning
3. Stereotyped and repetitive use of language or idiosyncratic language.
Students with ASD may exhibit stereotypical (i.e. use of nonsense words or phrases or
verbal fascinations) and repetitive or idiosyncratic language (i.e. contextually irrelevant
or not understandable to the listener due to a private meaning). Evidence of
stereotyped, repetitive, or idiosyncratic language may include, but is not limited to, the
following:
• Repeating words or phrases over and over
• Repeating what others say (echolalia) either immediately after the person said it or
at some time in the future
• Repeating television or movie lines, song lyrics, or other media that are out of
context and add no meaning to the conversation
• Use of words with a private meaning that only makes sense to those who are familiar
with the situation where the phrase originated (e.g. every time the student enters
the room he states, “That’s right on the money!”)
• Talking about a specific topic incessantly and out of context
• Overly formal use of words or expressions in conversation
The Michigan Autism Council 9 www.michigan.gov/autism

4. Lack of varied, spontaneous make-believe play or social imitative play
appropriate to developmental level.
Spontaneous make-believe play is a precursor to the use of symbols and corresponds
with language development. Social imitative play is also thought to be an early sign of
social reciprocity. Evidence of the lack of these behaviors may include, but is not limited
to, the following:
• Lack of spontaneous pretend play with toys (e.g. using objects only as they are
intended)
• Little elaboration on learned play schemes
• Lining up toys like cars or trains, stuffed animals, or action figures
• Focusing on only a part of the toy rather than actually playing with it (e.g. wheels on
a toy car or train, the string of a pull toy) or focusing on the movement of the toy
rather than the purpose of the toy; stacking blocks but not building anything
• Lack of finger play (e.g. “Itsy Bitsy Spider”) imitation without specific teaching and
prompts
• Limited play repertoires compared to peers (e.g. only plays with one specific toy or
item)
• Lack of advancement of play repertoires over time (e.g. still playing with Thomas the
Tank Engine while peers have moved on to LEGO® or board games)
• Rather than playing, directing peers to their assigned role in play
• Engages in construction play (e.g. puzzles, building blocks, assembling Transformers,
LEGO® bricks, setting up elaborate train track layouts) at the exclusion of flexible
representational play
Restricted, Repetitive, and Stereotyped Behaviors
Students with ASD engage in restricted, repetitive, and stereotyped behaviors that are
extreme and often interfere with other more appropriate behaviors or learning. Because
students with ASD are driven to engage in these behaviors, they are difficult to stop or
control. Further, disrupting the behaviors often causes significant distress for the student.
According to MARSE, restricted, repetitive, and stereotyped behaviors must include at least
one of the following:
1. Encompassing preoccupation with one or more stereotyped and restricted
patterns of interest that is abnormal either in intensity or focus.
Students with ASD can display intense interests and preoccupations that are intrusive,
reoccur frequently, and interfere with participation in daily activities. Limited access,
interruption, or removal of the activity or interest often causes significant distress.
Evidence of preoccupations and interests that are abnormal in intensity or focus may
include, but is not limited to, the following:
The Michigan Autism Council 10 www.michigan.gov/autism

• Talking about a particular topic (e.g. The Weather Channel) incessantly without
regard to the conversational partner
• “Playing” with the same toy over and over again and in the same way each time
• Incessantly seeking access to or talking about seemingly typical interests for age
such as video games (e.g. Minecraft), topic areas (e.g. anime), and characters (e.g.
SpongeBob or The Simpsons) but to the exclusion of most other topic areas or
activities
• Using a specific video game, television show, or movie as the lens through which
experiences or the world are viewed
• Excessively seeking access to or talking about atypical interests such as historical
events (e.g. Siege of Malta), specific appliances (e.g. coffee machine or fan), or
unusual types of animals (e.g. white Siberian tiger)
• Excessively seeking access to or talking about interests atypical for age (e.g. the
digestive system at age 4 or Thomas the Tank Engine at age 15)
2. Apparently inflexible adherence to specific, nonfunctional routines or rituals.
Students with ASD seek predictability in their environments and thus may create and
follow nonfunctional routines or rituals or have extreme distress when their routines are
altered. Evidence of inflexible adherence to nonfunctional routines or rituals may include,
but is not limited to, the following:
• Wearing a specific clothing item for a specific day or activity
• Rigid adherence to specific sequences in routines (e.g. eating food in a specific order,
completing worksheets from the bottom or right side only)
• Excessive and time consuming routines (e.g. bathroom, dressing)
• Distress when daily routines and schedules are altered
• Alphabetizing videos by the last name of the producer
• Having unusual self-imposed rules (e.g. must pass three red cars before entering
school)
• Insistence that others follow rules, including rules made up by the student
3. Stereotyped and repetitive motor mannerisms (e.g. hand or finger flapping or
twisting, or complex whole-body movements).
Some students with ASD engage in repetitive motor mannerisms, often called self-
stimulatory behaviors. Self-stimulatory behaviors occur in other disabilities as well, so it
is crucial for multidisciplinary evaluation teams to consider this item in context to the
other criteria. Evidence of stereotyped and repetitive motor mannerism may include, but
is not limited to, the following:
• Preoccupation with fingers, spinning, and twirling objects or self
• Pacing in a particular manner or routine
• Smelling, chewing, or rubbing objects in a particular manner
• Rocking or lunging
• Persistent grinding of teeth
• Repeated visual inspection of objects
The Michigan Autism Council 11 www.michigan.gov/autism

• Self-injurious behaviors including head-banging, hand biting, and excessive self-
rubbing and scratching
4. Persistent preoccupation with parts of objects.
Students with ASD can become preoccupied with parts, objects, or processes. The
fixation may appear to be more focused on how an object, including toys, actually works
instead of the function that it serves. Evidence of persistent (i.e. occurring over a
prolonged period of time) preoccupation with parts of objects may include, but is not
limited to, the following:
• A fascination with a specific part of the dishwasher or vacuum cleaner
• Spinning the wheels of a car
• Watching several seconds of a movie or cartoon over and over again, without
watching the complete movie
• Completing complex puzzles with more interest in putting the pieces together than
the puzzle picture as whole
Unusual or Inconsistent Response to Sensory Stimuli
Students with ASD may seek or avoid certain sensory stimuli to a degree that it interferes
with daily activities. Specific sensory areas can include sight, touch, hearing, smell, taste,
and movement.
According to MARSE, determination of ASD may include unusual or inconsistent responses
to sensory stimuli, but to be eligible under ASD, the student must also meet the other three
domains of eligibility. Sensory challenges alone are not sufficient to identify the student as
ASD because sensory issues can be found in a number of other eligibility areas. Conversely,
the absence of sensory challenges does not exclude a student from meeting ASD eligibility
criteria. As such, the evaluation team should analyze the child’s response to sensory stimuli
as it impacts the three domains of ASD eligibility (i.e. reciprocal social interaction,
communication, and restrictive and repetitive behaviors).
Age
According to MARSE, ASD typically manifests before 36 months of age. A child who first
manifests the characteristics after age three may also meet criteria, although generally the
child should have indicators of developmental differences by 36 months of age.
Adverse Impact
Determine if the ASD has an Adverse Educational Impact
According to MARSE, in order to be eligible for special education programs and services, a
student’s disability (i.e. ASD) must adversely affect educational performance in academic,
behavioral, or social domains. As such, a student may meet the eligibility criteria for ASD
but not be eligible for special education because access and progress in the general
education curriculum or environment is not affected by the ASD.
The Michigan Autism Council 12 www.michigan.gov/autism

Traditionally, multidisciplinary evaluation team members used the impact on the academic
domain alone as a determining factor in educational impact; however, for eligibility under
ASD, a student can have impact in any one of these three domains. A description of each
domain and the behaviors associated with them is provided below:
Academic
Determining adverse educational impact in the academic domain requires a review of the
student’s ability to meaningfully participate and progress in the general curriculum.
Evidence of academic impact may include, but is not limited to, the following:
• Delayed academic skill acquisition (e.g. reading, math, writing)
• Limited participation and engagement in instruction
• Lack of initiation and completion of school and home work
• Low grades and scores on academic assessments
Behavioral
Determining adverse educational impact in the behavioral domain requires a review of any
behavioral challenges that interfere with the student’s ability to meaningfully participate and
progress in the general curriculum or integrated environments (e.g. classroom, hallways,
lunch room, bus). Evidence of behavioral impact may include, but is not limited to, the
following:
• Aggression (e.g. hitting, kicking, spitting)
• Temper tantrums (e.g. dropping to the floor, crying, screaming)
• Disruptions (e.g. yelling, loud insistence that others are wrong and the student is right,
noises such as barking and humming)
• Non-compliance (e.g. not completing work or assessments, not following directions)
• Self-stimulatory behaviors (e.g. rocking, repetitive language, flapping)
• Eloping (e.g. running away, leaving the environment, hiding)
Social
Determining adverse educational impact in the social domain requires a review of the
student’s social interaction skills, relationship development, and engagement in the social
environment. Evidence of social impact may include, but is not limited to, the following:
• Difficulty making and keeping friends
• Challenges with reciprocal social interaction
• Difficultly understanding the perspectives of others (e.g. asks impolite questions; insists
on getting needs met even if someone nearby is upset; insists on always being first in
line; insists on winning all games)
• Obsession with peers following the rules (e.g. tattling on every infraction)
• Difficulty working cooperatively in groups
• Lack of independence in daily routines
• Transition challenges
The Michigan Autism Council 13 www.michigan.gov/autism
Need for Special Education Programs
and/or Related Services
According to the regulations for implementing the
Individuals with Disabilities Education Act (IDEA), to
be eligible for special education services, the
educational impact of the student’s ASD must
necessitate special education programs and/or related
services (§300.306). Special education is defined in
§300.39 as specially designed instruction.
The regulation further defines specially designed
instruction as “adapting, as appropriate to the needs
of an eligible child… to address the unique needs of
the child that result from the child’s disability.”
For example, specialized instruction must be needed for the student to make progress in
school and benefit from general education instruction to be eligible for services; having the
disability alone does not guarantee eligibility. Effectiveness of previously implemented
interventions is one way to determine the need for specialized instruction.
Education-based Evaluation for ASD
An education-based evaluation for ASD and recommendation of eligibility should not be
made based on any single evaluation component (e.g. interview, observation, test scores),
but rather each piece should be viewed as data to complete the evaluation picture.
Once the data is collected, the multidisciplinary evaluation team, using the preponderance
of evidence, makes a recommendation about whether or not the student meets the three-
pronged eligibility criteria:
1. The student meets the MARSE eligibility criteria for ASD,
2. The ASD adversely affects the student’s educational performance in academic,
behavioral, or social domains, and
3. The impact requires and necessitates special education services.
In addition to meeting the three-pronged eligibility requirements, the multidisciplinary
evaluation team must also gather information to assist in developing the Individualized
Education Program (IEP). This could include information such as:
• Communication needs of the student, including assistive technology
• The student’s social needs, including peer to peer support
• The student’s behavioral needs, including the need for a functional behavioral
assessment, positive behavioral support plan, and/or emergency crisis plan
“There is no single behavior
that is always typical of
autism and no behavior that
would automatically exclude
an individual child from a
diagnosis of autism.”
—National Research Council, 2001
The Michigan Autism Council 14 www.michigan.gov/autism
• Academic needs of the student, including accommodations and differentiation
Further, the multidisciplinary evaluation team is required to consider all suspected
disabilities. As such, a full and individual evaluation should include information to assist in
making differential eligibility recommendations (e.g. cognitive impairment, emotional
impairment, learning disability) if these disabilities are suspected.
Before beginning the eligibility determination process, a multidisciplinary evaluation team
(MET) must be established. Minimally, MARSE requires that the MET be comprised of a
psychologist/psychiatrist, school social worker, and authorized provider of speech and
language services. Although additional multidisciplinary evaluation team members can be
utilized, they are not required.
Additionally, some districts have opted to use a systematic team configuration model to
build capacity among staff and address specific challenges that may arise in some
evaluations. A description of the optional team configurations can be found in Appendix B.
The multidisciplinary evaluation team should function as a coordinated unit throughout the
evaluation process, regardless of the configuration or model used.
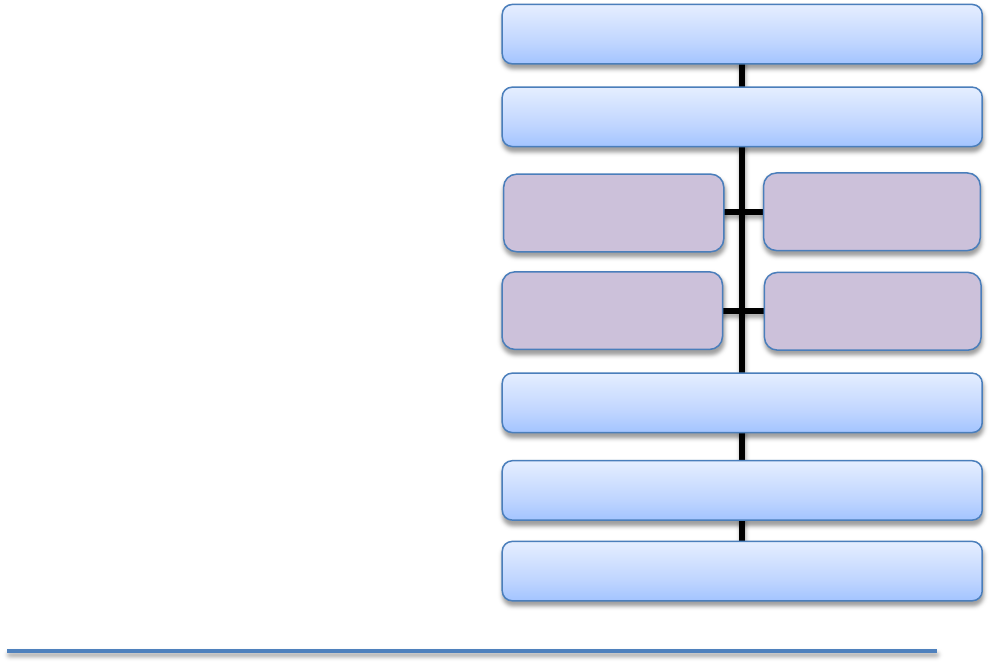
Education-based Evaluation Process for ASD
Below is an example of a process that districts may want to consider as part of the
multidisciplinary evaluation. Districts have found this process to be helpful in determining
whether or not a student meets eligibility criteria as a student with ASD.
Education-based Evaluation
Process for ASD
• Review of Existing Evaluation Data (REED)
• Completion of Evaluation Components
Teacher and Building Staff Interviews
Parent/Family Interview and Home Visit
Observations Across Settings by all
Team Members
Standardized Assessment
Considerations
• Results Review Meeting
• Evaluation Team Report
• Individualized Education Program (IEP)
Review of Existing Evaluation Data
Completion of Evaluation Components
Standardized
Assessment
Considerations
Results Review Meeting
Evaluation Team Report
Individual Education Program (IEP)
Parent/Family
Interview & Visit
Teacher/Building
Staff Interviews
Observations by all
Team Members
The Michigan Autism Council 15 www.michigan.gov/autism

Review of Existing Evaluation Data (REED)
IDEA §300.305 requires multidisciplinary school teams to conduct a REED for all special
education reevaluations. However, a REED is also an option for an initial evaluation,
especially if evaluation data from outside sources are available (e.g. diagnostic reports from
a private clinic, Community Mental Health). The REED can be used to:
• Review available information and assessment data (e.g. clinical diagnostic reports; other
medical reports);
• Determine if the information is sufficient to make a determination of eligibility
(i.e. meets eligibility criteria that impacts academic, behavioral, or social progress in
school that necessitates special education);
• Determine what else is needed to make a determination of eligibility (e.g. observations
to determine impact on educational performance); and
• Establish a plan for gathering the additional information.
For students with a clinical diagnosis of ASD, especially those who are also receiving private
or public insurance benefit services, school teams can expect to receive reports that include,
at minimum, a developmental history and standardized test scores. As such, this
information may not need to be repeated. However, IEP teams are also required to
determine whether the student meets the MARSE eligibility criteria for ASD as well as
determine the impact and necessity for special education services; it is likely that school
observations, teacher interviews, and/or direct assessments may still be needed.
It is important to note that the REED process can be used as a mechanism for increasing
collaboration among clinical and school assessment practitioners. Soliciting additional
information beyond what is provided in reports or inviting clinical staff to participate in the
REED process may enhance such collaboration.
When conducting a reevaluation, it is important to consider that MARSE defines ASD as a
“lifelong developmental disability.” As such, information to determine continued eligibility
should focus primarily on the impact of the ASD on access to and progress in general
education and the continued need for special education, rather than the eligibility criteria
itself. A full evaluation for the presence of ASD is likely necessary only when there is a
potential change in eligibility or the ASD eligibility is questioned.
Completion of Evaluation Components
The ASD Evaluation Component Checklist
A carefully designed evaluation plan supports the coordination of activities of the
multidisciplinary team evaluation. An evaluation checklist can be used to ensure timely
completion of components of the evaluation plan. Teams may want to consider completing
an evaluation component checklist as part of the REED process, and an example is provided
in Appendix C. Should all members of the evaluation team not be present at the REED
meeting, teams may want to consider a separate meeting shortly thereafter to complete the
checklist.
The Michigan Autism Council 16 www.michigan.gov/autism
Teacher and Building Staff Interviews
Education-based evaluations include an interview with the student’s teacher(s) and current
education-based provider(s). Because one of the goals of the education-based evaluation is
to understand how the suspected ASD affects a student in the course of the school day,
including the impact on progress in general education and the need for specially designed
instruction, it is important to obtain information from teachers and others who interact with
the child in the school context (Klin, et al., 2000).
There are a number of options for obtaining building staff input, including utilizing
commercially available checklists, rating scales, or other interview tools. While these may be
useful as part of the evaluation process, they frequently do not align with the MARSE
eligibility criteria and as such should not take the place of direct interviews tailored to the
individual student with a focus on information related to the MARSE eligibility criteria.
Additional options for gathering evaluation information include a facilitated meeting or face-
to-face interviews.
Facilitated Meeting
This option involves scheduling an intake meeting with relevant staff (e.g. teachers,
principal, service providers) facilitated by a member of the evaluation team. A meeting
format allows for rich, efficient discussion among participants about the student’s behavior
in the school context and provides opportunity for participating evaluation team members to
ask specific questions of the staff.
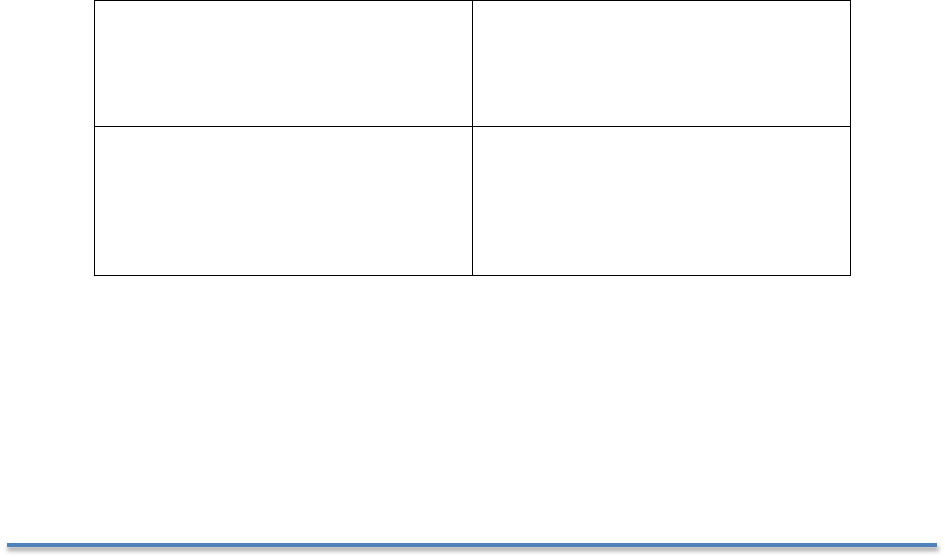
To ensure the discussion stays focused on information needed for eligibility determination,
the facilitator draws a quadrant like the one identified below on a white board or chart
paper, and then initially poses a broad statement, such as “Tell me about <student
name>,” to open the discussion.
Reciprocal Social Interaction
Communication
as it relates to ASD
Restrictive, Repetitive
& Stereotypical Behaviors
OTHER relevant impacting
factors including Sensory,
Cognitive Functioning,
Academic
It is important for the facilitator and other evaluation team members to allow the staff to
initially share any information that they feel is relevant and not limit their input. The
facilitator’s role is to capture all the information provided in the relevant quadrants, plus
anything falling under “other.” As the intake meeting progresses, the evaluation team
members can begin asking follow up questions to elicit more specific information to fill the
quadrants. Because the behaviors displayed by a student with ASD often fall into multiple
The Michigan Autism Council 17 www.michigan.gov/autism

quadrants, the absence of information in any one of the quadrants may be an indication
that the evaluation team should consider alternative areas of special education eligibility.
Face to Face Interviews
Another option for gathering staff information is to have two evaluation team members
conduct individual interviews with relevant staff. Having two members participate allows one
to lead the interview while the second takes notes in a quadrant document (as previously
described) and ask clarifying questions as needed.
The interview can begin much like the facilitated meeting with an open-ended question like
“Tell me about <student name>” or “What does <student name> do that makes you think
he has ASD (or another area of disability)?” The interview can then continue with follow up
and additional questions. Example interview questions and talking points are provided in
Appendix D.
Parent/Family Interview and Home Visit
Education-based evaluations also include an interview with the parent(s) or guardian(s) in
the family home when the student is there. If using this model, at least two team members
would be assigned to conduct the parent interview and home visit. An advantage of a home
visit is that it not only provides another observation setting, but it also helps team members
begin establishing rapport with the family.
Further, seeing reported home behaviors in the environment when they occur can assist the
evaluation team in differential eligibility decisions, as some behaviors attributed to ASD may
be explained by another disability when directly observed. For example, if a parent reports
that a child repeats words over and over, one might attribute this behavior to repetitive
language or echolalia. However, when observed in the home, this behavior could appear
more related to the child wanting something like a cookie and the parent not attending or
responding to the child’s request so he continually repeats the request. Having third party
observers confirm such behaviors can assist in eligibility decisions and also allow the
multidisciplinary evaluation team to better explain these behaviors and perhaps offer
intervention ideas to the family.
During a parent interview a critical question to ask the parents early in the interview is,
“What makes you think your child has ASD?” This may assist the multidisciplinary
evaluation team in sorting out information from the family that may be related to ASD from
other disability areas. For example, parents may indicate that they believe their child has
ASD because he or she has delayed or impaired communication skills. It is important to
highlight this concern within the evaluation process and address it in the evaluation report,
whether or not the student is determined eligible for special education under ASD. Examples
of parent interview questions and developmental history items can be found in Appendix D.
Observations Across Settings by all Team Members
Direct observations in a variety of natural contexts (e.g. classroom, hallway, lunch room,
recess) and across several days provide valuable information. Comprehensive observations
can provide a more accurate picture of how the student communicates, interacts, and
responds to varying stimuli and demands as compared to peers, and consistent behavioral
The Michigan Autism Council 18 www.michigan.gov/autism

patterns across observations increase the validity of the presence or absence of relevant
behaviors.
Observing the student in the school context also provides information about the impact of
the suspected ASD on the student’s progress in the general education curriculum and
settings relative to academic, social, and/or behavioral domains. Multiple observations can
further aid in the determination of the need for specially designed instruction and provide
valuable information for the development of the IEP (e.g. Present Level of Academic
Achievement and Functional Performance (PLAAFP) statement, supplemental aids and
services, goals and objectives).
An important consideration in conducting observations is making opportunities to engage in
activities with the student rather than sitting in the background taking notes. This type of
integrated observation will provide the observer greater opportunities to understand and
consider underlying motivations and immediate contextual variables that may be impacting
the presence of behaviors. This type of investigation is crucial for making differential
eligibility decisions as noted in a subsequent section of this document.
In addition, quantitative data should be collected within the qualitative observation process.
This will highlight the intensity of behaviors and provide further support for the impact and
need for special education. For example, when observing the student’s social interactions,
data can be collected on the frequency of spontaneous initiations with peers and adults as
compared to other students or the number of verbal, visual, or physical prompts needed to
complete classroom routines that peers complete independently. Observation considerations
and data collection templates are available in Appendix E.
Standardized Assessment Considerations
As stated previously, no single assessment method is sufficient for determining special
education eligibility for ASD. The multidisciplinary evaluation team must utilize information
gathered from multiple sources and methods and apply each to the components of the
MARSE criteria. Commercially available standardized assessment tools (e.g. norm-
referenced tests, checklists, and rating scales) may provide relevant information in making
clinical diagnoses of ASD and may actually be required for some diagnoses (e.g. ADOS for
ASD insurance benefit eligibility), but these measures are not based on the MARSE criteria
and thus are not sufficient in making eligibility decisions.
Further, students with ASD often exhibit characteristics (e.g. communication deficits,
difficulty with engagement, challenging behavior, and social reciprocity deficits) that make
assessment challenging and may negate the accuracy of the test results. Below is a list of
common behaviors that interfere with standardized assessment results for students with
ASD:
• Difficulty establishing rapport with the examiner
• Lack of motivation to please the examiner (e.g. deficits in reciprocity)
• Challenges with attention, engagement, and persistence in task demands
• Difficulty transitioning from one activity to another
• Language deficits that make it difficult to understand and follow instructions
The Michigan Autism Council 19 www.michigan.gov/autism

• Stimulus over-selectivity (e.g. attending to irrelevant stimuli)
• Interfering and challenging behaviors
Given these challenges, if the multidisciplinary evaluation team uses standardized
assessment tools, it is critical to report interfering behaviors and identify to what extent the
results of the assessment may not be accurate or reliable. These behaviors can, however,
provide helpful information in understanding the student’s response to stress and
frustration, interpersonal relationships, and communication.
For any standardized measures used in an education-based eligibility determination, the
multidisciplinary evaluation team should provide a rationale for its use. As such,
multidisciplinary evaluation teams should not have a predetermined battery of tools, but
rather determine their use on an individual basis and provide a clear purpose and intent for
using the tool in that particular evaluation (e.g. it answers a specific question that other
assessment methods do not). Teams should also report the technical adequacy of any tool
used including its reliability and validity. Although a complete review of the standards of
technical adequacy of standardized tools is outside the scope of this document, a brief
description is provided in Appendix F.
School teams should also consider the use of standardized tools that may be needed to
make differential eligibility decisions as well as determine the impact of comorbid conditions
on school performance. Caution should be given, however, to the impact of suspected ASD
on resulting scores. For example, school teams may presume that a cognitive score on a
standardized tool is an accurate reflection of ability, and thus consider eligibility under
Cognitive Impairment, when this score is frequently inaccurate for students with ASD due to
the challenges described previously.
To assist evaluation teams in determining if a particular standardized assessment tool
should be utilized, below is a set of questions to consider:
• Does the tool have adequate technical adequacy for making eligibility decisions related
to the suspected disability?
• What is the purpose or intended outcomes of using the tool?
• What questions are you attempting to answer by using the tool, and will the tool provide
that information? Is the information necessary and useful in making the eligibility
decision?
• What are the language requirements of the test, and do they match the ability level and
communication modality of the student?
• Given the student’s behavioral challenges, will the tool likely produce reliable and valid
results?
• How current is the tool (i.e. when was it published and standardized)?
• What are the potential challenges in using the tool (e.g. results are not consistent with
other information)?
Other than using standardized tools as designed, however, evaluators can use these
instruments to gather information about performance under various conditions (e.g. use of
accommodations and visuals supports) or to artificially create conditions that may not be
The Michigan Autism Council 20 www.michigan.gov/autism
easily observed in naturally occurring settings (e.g. responses to someone’s emotional
state).
Such expansions of the use of standardized tools can be beneficial in capturing rich
information on the student’s learning needs, strengths, and challenges. Also called
“breaking standardization,” it is important to remember that such changes to the
administration of the tool invalidate the scores obtained. This can be avoided for some tools
by first administering the test under standardized conditions and then “testing the limits” to
gain additional information. Some options for breaking standardization include the following:
• Administer subscales or items within subscales in a different order so highly preferred
tasks can follow less preferred ones to increase motivation
• Start at the beginning of a particular subscale (easiest item) rather than the age-
suggested starting point to create behavioral momentum
• Take frequent breaks
• Use tangible reinforcers
• Use a multiple-choice or fill-in-the-blank format rather than an open-ended style
• Paraphrase instructions or simplify language to match the child’s language level
• Use terms and phrases that are familiar to the child (e.g., “match” vs. “find me another
one just like this”)
• Use generic verbal prompts (e.g. for a picture vocabulary task, ask: “What is this? This
is a ______.”)
• Use visual supports to aid in the comprehension of instructions
Results Review Meeting
An education-based evaluation may include a summary meeting of the multidisciplinary
evaluation team. Once all of the observations and interviews have been conducted and all
evaluation data collected, the evaluation team may come together to review the
information. The purpose of this optional meeting is to collectively reach a team decision
regarding a recommendation of eligibility, as well as to begin formulating an impact and
need statement that can serve as the basis for the development of the IEP. Although there
may be multiple ways to conduct such a meeting, an example that addresses the challenges
often associated with decision-making is outlined below.
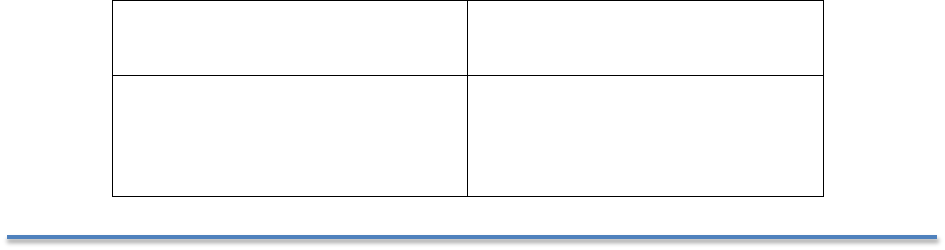
Scheduling a facilitated face to face meeting with the evaluation team (i.e. Results Review
Meeting) allows for a comprehensive and robust discussion from which a recommendation of
eligibility can be most accurately and reliably determined. During such a process, one
member of the evaluation team serves as facilitator and begins by drawing a table on a
white board or chart paper with the following labels:
Reciprocal Social Interaction
Communication
as it Relates to ASD
Restricted and
Repetitive Behaviors
OTHER relevant impacting
factors including Sensory,
Cognitive Functioning,
Academic
The Michigan Autism Council 21 www.michigan.gov/autism

Multidisciplinary evaluation team members then begin to discuss the information obtained
through parent and staff interviews, observations, and any other methods, while the
facilitator lists the information in the appropriate areas in the chart and a note-taker
captures the information in a report template. Some teams have found it helpful to color
code the information based on the source (e.g. parent, teacher, evaluation team) or other
relevant variables. Once all of the information is listed on the board, the team uses the
preponderance of the evidence available to answer the eligibility criteria questions:
Relative to the required number of criteria needed in each broad category:
• Is there a qualitative impairment in social interaction?
• Is there a qualitative impairment in communication?
• Is there the presence of repetitive, restricted, and stereotyped behaviors?
If the answer to any one of these questions is “no,” the student does not meet the MARSE
eligibility criteria for ASD. However, if this is the case, the possibility of eligibility in another
disability category should be considered.
If the answer to each question is “yes,” the MARSE ASD eligibility criteria are met and the
team can go back and identify specific criteria that best represent each category. As a
reminder, in order for the criteria to be met, at least two items must be present in the
reciprocal social interaction area—one in communication, and one in restricted and
repetitive behaviors.
In addition to meeting the MARSE ASD eligibility criteria, the ASD must have an adverse
impact on the student’s academic, social, or behavioral progress and the student must
demonstrate a need for specially designed instruction.
Should impact and need exist, the team can begin to develop a relevant statement that can
serve as the initial foundation for the PLAAFP. To begin this discussion, posing the question,
“What about the student’s ASD is getting in the way of access to and progress in the
general education curriculum and environments?” will assist the team in staying focused on
impact and need versus generating a list of skill deficits.
The last task for the evaluation team to complete during the Results Review Meeting is to
review the evaluation checklist and confirm those team members that will be providing
feedback and recommendations to parents, school staff, and other relevant stakeholders
prior to the IEP, as well as determine which multidisciplinary evaluation team members will
be attending the IEP.
Multidisciplinary Evaluation Team Report
To ensure a clear and concise report that identifies the presence or absence of critical
eligibility characteristics, avoids conflicting information across evaluators, and builds an
accurate case for the conclusions of eligibility, the multidisciplinary evaluation team may
integrate all assessment information into one combined report according to and following
the MARSE criteria.
The Michigan Autism Council 22 www.michigan.gov/autism

The report can explain in detail any and all observation data or other assessment
information that does not align with the conclusions of eligibility. For example, if, during an
interview, the parent reports that the student repeats words constantly (as described in the
Parent/Family Interview and Home Visit section), the report should describe how and why
these behaviors do not support the conclusion of ASD and provide an alternative
explanation for the behavior.
The optional combined report should also include information on the additional two prongs
of eligibility (i.e. impact of the disability on access to and progress in general education and
the need for specially designed instruction). This information will assist the IEP team in
developing a comprehensive PLAAFP and support the development of supplementary aids
and services, goals and objectives, and needed programs and services. An example report
template is provided in Appendix G.
Individualized Education Program
The final step is for the IEP team to determine whether the student meets the ASD eligibility
criteria. Should the student be eligible for special education programs and/or related
services, the IEP team will incorporate the information from the evaluation process to
identify the special education supports and services necessary for the student to receive a
Free and Appropriate Public Education (FAPE) in the Least Restrictive Environment (LRE).
Differential Eligibility Decision-Making
To make quality differential eligibility decisions, it is important for multidisciplinary
evaluation teams to understand disorders that mirror ASD and those that are comorbid with
the condition. A number of characteristics associated with ASD (e.g. poor eye contact,
hyperactivity, difficulty with focused attention, difficulty with transitions or changes in
routine, poor peer relationships, repetitive behaviors, delayed language and developmental
skills) are also seen in other developmental or mental health disorders (e.g. Attention
Deficit Hyperactivity Disorder, Learning Disorders, Cognitive Impairment, Reactive-
Attachment Disorder) (Sikora, 2008).
As such, students with these conditions may qualify under another MARSE eligibility
category (e.g. cognitive impairment (CI), learning disability (LD), emotional impairment
(EI), other health impairment (OHI)). Further, a number of conditions that represent other
eligibility categories are comorbid with ASD, such as CI and EI (specifically regarding
anxiety disorders and depression, in the case of EI). In fact, anxiety disorders and
depression are the primary comorbid conditions in ASD.
As such, it is important for multidisciplinary evaluation teams to review information that
may assist them in differentiating ASD from other disabling conditions. As described in the
Results Review Meeting in Appendix C, teams can use chart paper or a white board to
develop tables or concentric circles that allow them to compare and contrast information
such as:
The Michigan Autism Council 23 www.michigan.gov/autism

Eligibility Criteria
It is critical for evaluation teams to have a solid understanding of the other disabilities and
criteria outlined by MARSE in order to be able to effectively compare and contrast behaviors
and other assessment information within each disability.
Age of Onset of Characteristics and Developmental History
Although some developmental sequences appear similar across disabilities, it is important to
review and discuss the student’s developmental history to assist in differentiating one
disability from another. For example, students on the autism spectrum generally have early
developmental histories that include either the lack of the development of spoken language
not accompanied by attempts to compensate or advanced levels of language, especially in
interest areas. Students with other disabilities may have language deficits, but attempts to
use alternative methods to communicate are present.
Underlying Motivation or Function of Behaviors
Because behaviors can look similar across disabilities, it may help to collect information and
compare and contrast the underlying motivation of behavior, as this may give the
multidisciplinary evaluation team clues into whether one disability or another exists. For
example, refusals to follow expectations and aggression toward others can occur in students
who have ASD and those who are EI. However, in ASD these behaviors are often related to
deficits in social reciprocity or communication skills, and/or a lack of theory of mind,
whereas for students with EI, this may be related to emotional dysregulation, deficits in
self-worth, or a lack of connecting with others as a child (e.g. Reactive Attachment
Disorder).
Additionally, behaviors related to Social Maladjustment, which is an exclusionary factor for
EI, may be seen in students with ASD (e.g. behaviors that violate socially acceptable rules,
not accepting responsibility for actions, or not demonstrating remorse). However, for
students with ASD, these behaviors are related to the deficits described previously as
opposed to behaviors related to conduct disorder or antisocial disorder, which is often the
case for students with Social Maladjustment. For example, the team may need to
distinguish between not caring about social rules and not understanding that social rules
change from situation to situation. They may also need to distinguish between apparent lack
of remorse due to not caring about others’ feelings as opposed to not understanding that
others have different feelings.
History of Interventions
It is important for multidisciplinary evaluation teams to know what interventions are more
likely to be effective for students with one condition versus another. For example, visual
schedules and supports are considered universal supports for students with ASD because
they are an effective way to help the majority of those students increase engagement with
tasks. However, for a student with a conduct disorder, a visual schedule may not always be
as effective.
Once the multidisciplinary evaluation team compares and contrasts relevant variables
associated with the differential eligibility decision, a final recommendation of eligibility must
be made. The most important component of making this final decision, especially for
The Michigan Autism Council 24 www.michigan.gov/autism
students who may meet the criteria in one or more MARSE eligibility areas, is determining
which disability most impacts access to and progress in general education and requires
specially designed instruction. In most cases, if the student meets the eligibility criteria for
ASD but has a common comorbid condition related to ASD (e.g. anxiety, depression) that
could result in another eligibility consideration (e.g. EI), the ASD would typically be
considered the primary disability.
In making this final eligibility decision, it is often helpful for multidisciplinary evaluation
teams to remember that, for some students with complex presentations of their disability,
there will always be instances of behavior that doesn’t fit or align perfectly. As such, the
multidisciplinary evaluation team’s role is to determine, using the preponderance of
evidence, which eligibility is the most representative of the one that is impacting access to
and progress in general education.
Considerations for Evaluation of Young Children
Given the complexities and range of developmental changes in young children, it is critical
for multidisciplinary evaluation team members to have a solid understanding of the range of
typical development in early childhood and the disorders that mirror ASD in this population.
Consideration of development in the areas of communication, cognition, play, emotional and
social functioning, relationships with caregivers and peers, sensory-motor, and self-
regulation should be included in early childhood evaluations. Given that the range of
development can be broad, a higher threshold for determining communication and social
and behavioral impairment may need to be considered.
For example, if a two-year-old child displays a significant communication delay as well as
some difficulty with reciprocal social interactions, the multidisciplinary evaluation team
should consider whether the social difficulties are a result of the significant communication
delays rather than a presentation of a qualitative social impairment related to ASD.
Additionally, this same child may present with motor mannerisms such as hand-flapping
when excited, which for some children is part of the range of typical development. As such,
it would be quite a stretch to consider it representative of repetitive behavior that would
meet ASD criteria. In this scenario, the multidisciplinary evaluation team may determine the
child eligible for having a speech and language impairment (SLI) under R 340.1710 by
considering the social deficits a result of the communication delay and the hand-flapping
within the range of typical development. In this way, SLI is more representative of the
child’s current developmental profile.
Despite these considerations, it is not appropriate to recommend eligibility in another
category to prolong or avoid the ASD eligibility. If, after careful and comprehensive
assessment, the child fully meets the criteria for eligibility under ASD, the multidisciplinary
evaluation team must provide the recommendation of ASD eligibility to the IEP team. The
regular practice of finding a child eligible in the categories of R 340.1710 (“Speech and
language impairment” defined; determination) or R 340.1711 (“Early childhood
developmental delay” defined; determination) to “wait and see” if it is ASD should be
discontinued. According to MARSE, the early childhood developmental delay eligibility
The Michigan Autism Council 25 www.michigan.gov/autism

category should be used only when “primary delays cannot be differentiated through
existing criteria within [other eligibility categories].” In addition, policies that indicate age
cutoffs for finding a student eligible under the ASD classification should also be eliminated.
When considering evaluation for ASD in young children, it is also important for team
members to have a solid understanding of the unique presentation of ASD characteristics.
Although social deficits and delays in spoken language are the most prominent
characteristics evidenced by very young children with ASD (Stone, et al, 1999), there is
often confusion about typical development in the areas of pragmatic language, play, and
social behavior in young children.
Pragmatic Language
Pragmatic language refers to the ability to use new language skills in reciprocal social
interaction with peers. Around the age of four, typically developing children:
• Understand that they need to talk differently to their preschool teacher than to a peer
than to a younger child
• Understand the importance of getting another person’s attention before talking to them
• Use words to request things and communicate their approval and disapproval
• Direct their language to social interactions with adults and peers
• Verbalize out loud their “private speech” about their thoughts, feelings, and hopes as
they play and interact with others
It is important to observe for these behaviors or their absence when conducting early
childhood ASD evaluations.
Play
Observation during play with typical peers is highly recommended when conducting early
childhood evaluations for ASD. The following are guidelines regarding the typical
developmental sequence of play to consider:
• Object exploration—Explores an object, but does not assimilate how to use it in play
(e.g. child makes a stirring motion with a spoon and then drops it)
• As young as 16 months, directs play towards another person (e.g. picking up the
pretend cell phone, making a ringing sound, and handing it to a parent)
• Representational play—Uses “meaningless” objects in a creative way to play a role in
pretend play (e.g. block becomes a cell phone or a train)
• Parallel play—Between the ages of 18 months and three years, plays next to, but not
with, other children; may not appear to interact with but is very aware of the presence
of other children
• Around age three, play moves from objects to imaginary objects or beings (e.g. swing
becomes a spaceship, cup has pretend tea in it)
• Also around age three, begins to animate toys (pretends to feed a doll that is hungry)
• Between ages three and five, integrates more than one act into a sequence or story of
acts; is able to develop play themes with peers and incorporates others’ ideas into play
schemes
The Michigan Autism Council 26 www.michigan.gov/autism

Social
Socially, by age three, the parallel play that is characteristic of the interaction of the two-
year-old is replaced by social play with peers. This can center on shared interests, rough
and tumble play, as well as complicated schemes. By age four, most children prefer playing
with another child to playing alone, with social interactions with peers characterized by
talking, smiling, laughing, and playing. At age four, children begin to display Theory of Mind
and understand that other people may have thoughts, feelings, and ideas that are different
from their own (Leventhal-Belfer and Coe, 2004). As such, consideration of typical social
development must be included in determining social impairment in young children.
The Michigan Autism Council 27 www.michigan.gov/autism
Appendix A
Michigan Administrative Rules for Special Education
(MARSE) Criteria for ASD
R 340.1715 Autism spectrum disorder defined; determination.
(1) Autism spectrum disorder is considered a lifelong developmental disability that adversely
affects a student’s educational performance in 1 or more of the following performance
areas:
(a) Academic.
(b) Behavioral.
(c) Social.
Autism spectrum disorder is typically manifested before 36 months of age. A child who first
manifests the characteristics after age 3 may also meet criteria. Autism spectrum disorder is
characterized by qualitative impairments in reciprocal social interactions, qualitative
impairments in communication, and restricted range of interests/repetitive behavior.
(2) Determination for eligibility shall include all of the following:
(a) Qualitative impairments in reciprocal social interactions including at least 2 of the
following areas:
(i) Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye
gaze, facial expression, body postures, and gestures to regulate social interaction.
(ii) Failure to develop peer relationships appropriate to developmental level.
(iii) Marked impairment in spontaneous seeking to share enjoyment, interests, or
achievements with other people, for example, by a lack of showing, bringing, or
pointing out objects of interest.
(iv) Marked impairment in the areas of social or emotional reciprocity.
(b) Qualitative impairments in communication including at least 1 of the following:
(i) Delay in, or total lack of, the development of spoken language not accompanied
by an attempt to compensate through alternative modes of communication such as
gesture or mime.
(ii) Marked impairment in pragmatics or in the ability to initiate, sustain, or engage
in reciprocal conversation with others.
(iii) Stereotyped and repetitive use of language or idiosyncratic language.
(iv) Lack of varied, spontaneous make-believe play or social imitative play
appropriate to developmental level.
(c) Restricted, repetitive, and stereotyped behaviors including at least 1 of the following:
(i) Encompassing preoccupation with 1 or more stereotyped and restricted patterns
of interest that is abnormal either in intensity or focus.
The Michigan Autism Council 28 www.michigan.gov/autism

(ii) Apparently inflexible adherence to specific, nonfunctional routines or rituals.
(iii) Stereotyped and repetitive motor mannerisms, for example, hand or finger
flapping or twisting, or complex whole-body movements.
(iv) Persistent preoccupation with parts of objects.
(3) Determination may include unusual or inconsistent response to sensory stimuli, in
combination with subdivisions (a), (b), and (c) of sub-rule 2 of this rule.
(4) While autism spectrum disorder may exist concurrently with other diagnoses or areas of
disability, to be eligible under this rule, there shall not be a primary diagnosis of
schizophrenia or emotional impairment.
(5) A determination of impairment shall be based upon a comprehensive evaluation by a
multidisciplinary evaluation team including, at a minimum, a psychologist or psychiatrist, an
authorized provider of speech and language under R 340.1745(d), and a school social
worker.
The Michigan Autism Council 29 www.michigan.gov/autism
Appendix B
Team Considerations and Configurations
According to MARSE, the multidisciplinary evaluation team for ASD eligibility must include a
school psychologist or psychiatrist, school social worker, and authorized provider of speech
and language services. The ISD or LEA can choose to include others, such as the
occupational therapist (OT) or teacher consultant (TC), but they are not required.
Multidisciplinary evaluation teams that function as a coordinated unit throughout the
process produce an evaluation report that is integrated rather than several separate reports
by each member of the team under one cover. There are a number of special
considerations for team assignments based on how the ISD or LEA functions and the need
to address a variety of potential challenges or concerns. Examples include, but are not
limited to, the following:
Team Structure Examples
Benefits
Risks
A. Dedicated team to
conduct all evaluations
within ISD/district in
which ASD is suspected
• Team develops high level of
competency and deep
knowledge of ASD
• Consistency in evaluations
throughout the ISD/district
• Objective viewpoint of student
during evaluation process
• Does not build capacity around
evaluations for ASD eligibility
across staff
• Increased likelihood that team
will get called in for problem
solving because they hold the
expertise around ASD
• Evaluation load may overwhelm
availability of team
B.
Objective team that is
strategically identified
from pool of itinerant
staff when evaluation for
suspected ASD is
requested; team
members are not
assigned to building in
which student attends
school
•
Objective viewpoint of student
during evaluation process
• Allows for capacity building
across staff; staff more
experienced and knowledgeable
about ASD can be paired with
less experienced staff
• Allows for evaluation load to be
evenly distributed across staff
•
Requires coordination and
oversight for formation of teams
• May result in inconsistency
across evaluations
C. Evaluation for suspected
ASD is conducted by MET
members that are
assigned to building in
which student attends
school
• Those with more knowledge
about student conduct the
evaluation
• Team members who conduct
evaluation will likely be same
staff that provide potential
special education services
• Potential for evaluation team to
be influenced by political or
contextual influences
• Possible risk in having a
preconceived opinion of
eligibility prior to evaluation
The Michigan Autism Council 30 www.michigan.gov/autism
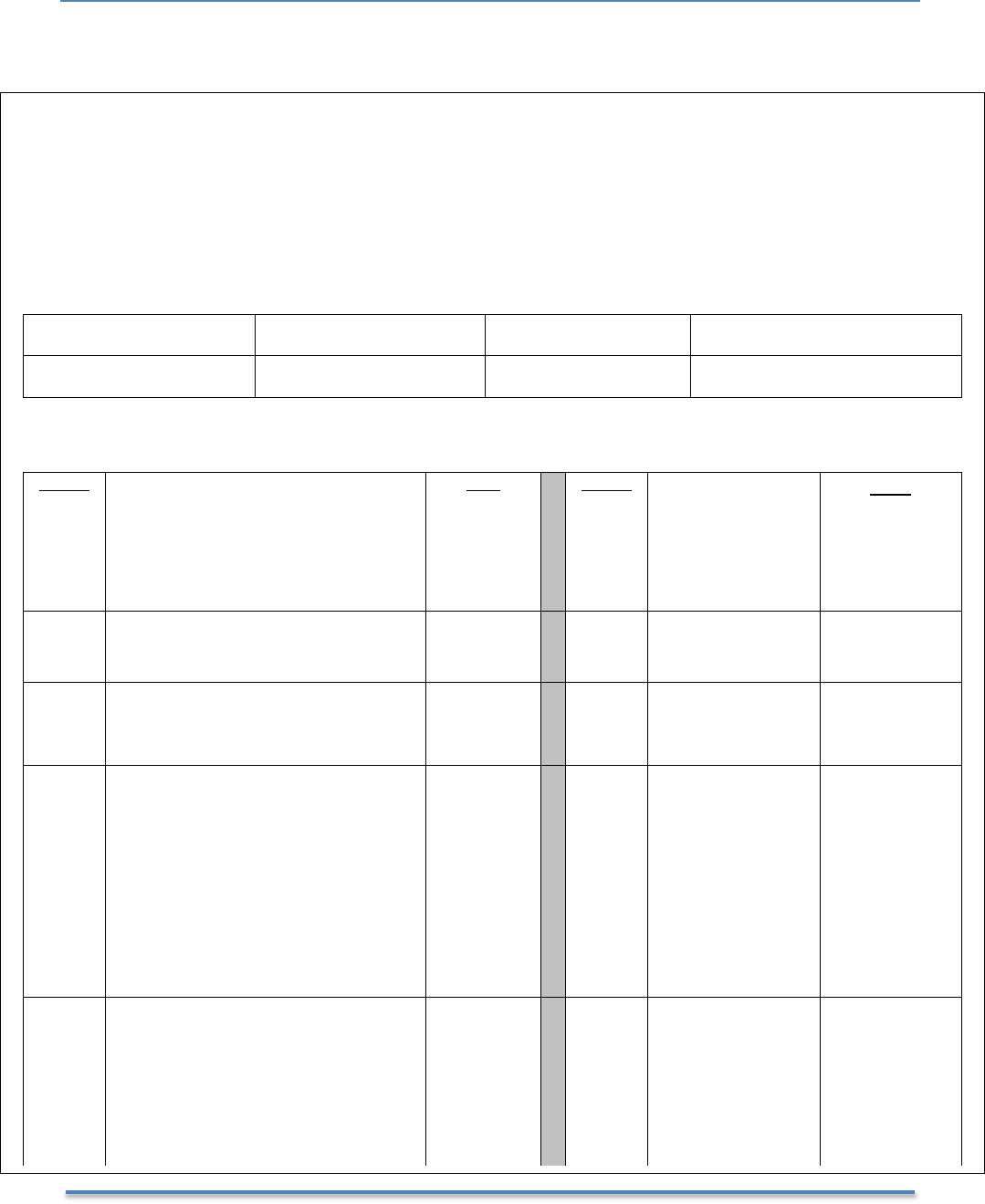
Appendix C
The ASD Evaluation Component Checklist
ASD Evaluation Component Checklist
Today’s Date: _____________________________
Team Members: Psych _______________________ SLP ___________________________
SSW _______________________ Other ___________________________
Team Leader: _____________________________
Name of Student
DOB
District/School
Due Date (Last IEP)
Evaluation Components
Date(s)
Teacher / Building Staff Interviews
• Teacher
• SLP
• SSW
• OT
•
OTHER
Who
Date(s)
Results Review
Meeting
Who
Educational History
CA 60 Review
Combined Written
Report Completed
Parent Interview
Home Visit
Provide Report
to Parent and
School Team
Observations Across Settings by:
• Psychologist
• SLP
• SSW
• OTHER
List Settings:
Attendee(s)
to the IEP:
Administrations of
Standardized Tools
List Tool(s):
OTHER TASKS
The Michigan Autism Council 31 www.michigan.gov/autism

Appendix D
Examples of Staff and Parent Interview Items
Whether a commercially available staff and parent interview form is used or one that is
created independently is used, it is important to consider the following talking points when
interviewing staff and families:
• Verbal and non-verbal communication including receptive language
• Pragmatics including initiating, maintaining, and ending conversations, conversational
turn-taking, topic maintenance, and conversational repair
• Social interaction with both peers and adults
• Sharing of achievements with others
• Interest in activities, interests, and achievements of others
• Play patterns and skills
• Areas of interest or expertise
• Adaptive skills (self-help skills and activities of daily living)
• Existence of established routines
• Movement and motor skills including repetitive movements/behaviors
• Student’s ability to handle change and transitions
• Idiosyncratic or unusual behavior
• Response to various types of sensory input
• Challenging behaviors
• Cognitive and learning style including strengths, processing time, attention to tasks,
concrete/abstract thinking, and learning new tasks or skills
• Concerns, issues
Although parent interview questions should relate to the MARSE criteria, it is also important
for making differential eligibility decisions to include information on the following:
• Medical history, including current health issues and medications
• Developmental history, including developmental milestones, when the family first had
concerns about the child’s development, and a list of those concerns
• Adaptive skills, including self-help skills and activities of daily living
• Educational progress, including adjustment to school, grades, attendance, favorite
subjects or activities, relationships with peers, problems and concerns, strengths, and
abilities
The Michigan Autism Council 32 www.michigan.gov/autism

Appendix E
Observation Considerations
While not required in state or federal law or rule, observations are an essential component
of an education-based evaluation for ASD. Below are observation tools, forms, and
considerations that may assist in gathering reliable data:
• Observe across a variety of settings (e.g. at home alone, at home with siblings or other
similar age peers, visiting other family members, preschool snack or play time, recess,
music, social studies, and lunch)
• Observe in the presence of different individuals (e.g. day care provider, teachers, peers,
and parent)
• Examine behavior under varied task demands (e.g. play time, small group, sharing,
independent activities, written work, large group work, unstructured activities)
• Observe at different times of the day (e.g. morning, afternoon, before/after lunch)
• If possible, observe during times of potential stress (e.g. new activity, changing from
playing with a favorite toy or activity, an unexpected change in routine, family or school
outing, instruction with a high level of verbal content, academic demands above
perceived instructional level, presence of a substitute teacher, situations that may
require additional problem solving)
• Observe for spontaneity and initiation of social behaviors rather than just noting the
student’s response to others
• During observations, note how others interact with and respond to the student
• When observing older students or those with high verbal skills, it may be necessary to
note more subtle manifestations of ASD (e.g. the student may attempt to socialize but
may be extremely naive, inept, or rote in his or her conversational skills and abilities;
some students may show imaginative play during observation, but parents or teachers
note that the same actions or play routines are repeated each time they use that specific
material)
• If conducting a direct assessment, take note of the presence or absence of relevant
behaviors; some students are very comfortable in testing situations and perform very
well while others are highly stressed
• Look for patterns as well as differences of performance across multiple variables; these
can provide valuable information concerning the characteristics of the student as well as
insights for developing interventions. Consider the environmental or assessment setting
as a critical component for understanding the student's behavior (e.g. proximity of
child/student to teacher, room arrangement, desk arrangement, lighting, noise levels)
• Note the antecedents and consequences that occur around the behavior; although the
antecedent-behavior-consequence (ABC) pattern is not always linear in ASD, taking note
of the context that occurs around the behavior can be invaluable in differentiating
between an ASD and an emotional or cognitive impairment
The Michigan Autism Council 33 www.michigan.gov/autism
Evaluation Team Observation Form & Probe Questions
Student’s Name: Observation Location: Date:
Reciprocal Social Interaction
Communication as it Relates to ASD
Nonverbal Behaviors
• Use eye contact to engage the conversational
partner?
• Use facial expressions to match the situation?
• Gesture to engage and influence?
• Demonstrate consciousness of physical proximity?
Peer Relationships
• Interact with peers in activities appropriate to
developmental level?
• Appear indifferent to peers?
• Engage in developmentally appropriate activities?
• Appear attuned to the subtleties of interactions
with peers?
Spontaneous Sharing
• Approach or seek out another person?
• Approach another person to share something of
interest?
Reciprocity
• Take turns during conversation?
• Show empathy to match the mood of peer?
• Exhibit tolerance of changes of topic?
• Show an awareness of the partner’s interests
during conversation or play?
Communicative Intent
• Respond to other people? Communicate to request or
protest?
• Gesture or take the hand of an adult to direct the adult
to a wanted item?
• Use eye gaze, vocalizations, facial gestures, signing, or
pictures to indicate wants?
Pragmatics
• Provide sufficient background or reference information to
partner to understand and participate in conversation?
• Use and react to nonverbal cues exhibited by others?
• Use vocabulary and knowledge base to express
emotions/feelings in a variety of situations?
• Understand and use non-literal language (e.g., idioms or
slang)?
• Discuss at length a single topic that is of little or no
interest to others?
Stereotyped/Repetitive Use of Language
• Display atypical communication such as echolalia,
perseveration, and pronoun reversals?
• Speak with flat, emotionless voice or with exaggerated
inflection?
• Repeatedly use a limited number of utterances?
Lack Varied Play
• Play with toys as intended?
• Recognize the play repertoire of peers has changed?
• Participate in age-appropriate play?
Restrictive, Repetitive, and
Stereotypical Behaviors
OTHER Relevant Impacting Factors
Preoccupation
• Exhibit an all-consuming, high interest in objects,
topics, or themes beyond typical developmentally
appropriate levels?
• Have a restricted or narrow range of interests,
including unusual interests, as compared to peers?
• Show difficulty letting go of perseverative thoughts,
activities, actions, or behaviors?
Inflexibility
• Use ritualistic actions or behaviors? Rigidity in
routine, difficulty with change and/or transitions?
• Display an insistence on sameness?
Stereotyped or Repetitive Motor Mannerisms
• Display repetitive motor or vocal patterns such as
flapping, rocking, pacing, humming, picking, or
chewing?
• Use self-injurious behavior?
Preoccupation with Parts of Objects
• Twirl, spin, and/or bang objects in a hyper-focused
manner? Fixate on how an object works rather than
its function?
Academic:
Cognitive Functioning:
Sensory Including Impact on the Three ASD
domains:
Characteristics Related to Other Disabilities:
The Michigan Autism Council 34 www.michigan.gov/autism
Student’s Name: Observation Location: Date:
Reciprocal Social Interaction
Communication as it Relates to ASD
Restrictive, Repetitive, and
Stereotypical Behaviors
OTHER Relevant Impacting Factors
Academic:
Cognitive Functioning:
Sensory Including Impact on the Three ASD
domains:
Characteristics Related to Other Disabilities:
Evaluation Team Observation Form
The Michigan Autism Council 35 www.michigan.gov/autism
Appendix F
Information on Standardized Assessments
Reliability refers to the degree to which an assessment tool produces stable and consistent
results. Although a number of reliability measures may be reported in test manuals, test-
retest reliability and inter-rater reliability are of particular importance.
Test-retest reliability ensures that a testing instrument produces similar results across two
different administrations, and inter-rater reliability assesses the degree to which different
raters or evaluators produce similar results. If a testing instrument cannot produce
consistent results over time or across evaluators, caution should be taken in using that
instrument to make diagnostic decisions.
Although good reliability is a necessary component of diagnostic tools, it is not sufficient in
determining their accuracy. For a test to be accurate, it must also be valid. Validity refers to
how well a testing instrument measures what it is purported to measure. For example, if a
scale is off by five pounds, it might read the weight correctly day after day, making it
reliable. However, because the scale is off by five pounds, it is not measuring true weight
and thus is not a valid measure.
Such is true of an assessment tool that purports to measure the characteristics of ASD.
Caution should be taken when using tools that are not adequately valid for identifying ASD.
Further, there are no tools that have been validated for use in determining education-based
eligibility.
Information on commercially available standardized tools and their technical adequacy can
be found at the Central Assessment Lending Library (CALL) at Central Michigan University.
These technical adequacy briefs outline the reliability and validity of a number of
standardized measures used in the assessment of ASD. Readers are referred to their site to
request copies of these briefs.
www.cmich.edu/colleges/chsbs/Psychology/call/Pages/default.aspx
To assist further in making decisions about the use of standardized assessment tools, below
is a list of common diagnostic measures used for identifying ASD. This is not an exclusive
list and does not represent a recommendation for their use. Readers should access the
technical adequacy information from CALL for each tool and then make independent and
individualized decisions about which tools should be used for any given evaluation.
The Michigan Autism Council 36 www.michigan.gov/autism
Modified Checklist for Autism in Toddlers Revised (M-CHAT-RF)
The M-CHAT is an expanded American version of the original CHAT from the UK. The M-
CHAT has 23 yes/no questions and may be used with children from 15 to 30 months old.
www.mchatscreen.com/Official_M-CHAT_Website.html
Autism Diagnostic Interview – Revised (ADI-R)
The ADI-R is a standardized interview for diagnosing autism. It can be used for children with
a mental age at or above two years. Administration time is 90-150 minutes, including
scoring.
www.wpspublish.com/store/p/2645/autism-diagnostic-interview-revised-adi-r
Autism Diagnostic Observation Scale (ADOS-2)
The ADOS-2 is a structured observation for diagnosing ASD. The tool includes several
modules based on the child’s language skills and can be used from 12 months through
adulthood. Administrative time is 40 to 60 minutes.
www.wpspublish.com/store/p/2648/autism-diagnostic-observation-schedule-second-edition-
ados-2
Autism Screening Instrument of Educational Planning – Third Edition (ASIEP-3)
The ASIEP-3 rates individuals from 2 years to 13 years and 11 months of age in five core
areas (behavior, vocal behavior, interactions, education, and learning rate). It is designed to
identify individuals with ASD as well as assist in planning and monitoring educational
programs for students with ASD.
www.proedinc.com/customer/ProductView.aspx?ID=4217
Childhood Autism Rating Scale-Second Edition (CARS-2)
CARS is a 15-item rating scale for diagnosing ASD. Ratings are based on frequency of the
behavior in question, its intensity, peculiarity, and duration. It may be used for children two
years and older. Administrative time is 5 to 10 minutes.
www.proedinc.com/customer/ProductView.aspx?ID=4754
Gilliam Asperger’s Disorder Scale-Second Edition (GADS-2)
The GADS is a norm-referenced assessment tool designed to evaluate individuals who may
have Asperger’s Disorder. Appropriate for individuals aged 3 to 22. Completion time is 5 to
10 minutes.
www.pearsonclinical.com/education/products/100000417/gilliam-aspergers-disorder-scale-
gads.html
Gilliam Autism Rating Scale (GARS-3)
The GARS-3 is based on the DSM-5. This rating scale may be used for identification and
diagnosis of individuals at or above age three. The instrument consists of 56 items
describing the characteristic behaviors of persons with autism. The items are grouped into
six subscales: Restrictive/Repetitive Behaviors, Social Interaction, Social Communication,
Emotional Responses, Cognitive Style, and Maladaptive Speech.
www.proedinc.com/customer/productView.aspx?id=5818
The Michigan Autism Council 37 www.michigan.gov/autism
Appendix G
Report Components with Descriptors
Multidisciplinary Evaluation Team (MET) Report
Date of Report:
Student Name: Date of Birth: School:
Evaluation Team:
Psychologist:
School Social Worker:
Authorized Provider of Speech & Language Services:
REASON FOR EVALUATION
Student was referred for an evaluation to determine eligibility for special education under the ASD
eligibility criteria by his present teacher due to challenges with (list reasons the referral was initiated).
ASSESSMENT SOURCES
Review of School Records
Review of Private / Medical Assessments and Reports (if applicable)
Parent Interview on (list date(s))
Teacher and Staff Interviews on (list date(s))
Classroom Observations on (list observers, dates, times and locations)
Administration of the following standardized tools:
The following information was gathered through review of records, observations, school staff and parent
interviews and surveys, review of previous assessment information, and direct assessment and rating
scales listed above. A summary of this information and relevant scores are provided within the context of
the Michigan ASD eligibility requirements below.
RELEVANT BACKGROUND INFORMATION
NOTE: Include only information that is relevant to making a decision of ASD eligibility, including, but
not limited to:
• Developmental history
• Private evaluations and report summaries
• School history including discipline issues, grades, etc.
• Previous MET evaluations or other eligibility history
• Include any information relevant to the eligibility criteria in the corresponding sections below:
The Michigan Autism Council 38 www.michigan.gov/autism
DETERMINATION OF SPECIAL EDUCATION ELIGIBILITY UNDER ASD
According to Michigan Administrative Rules for Special Education (MARSE), ASD is considered a
lifelong developmental disability that adversely affects a student’s educational performance in academic,
behavioral, and/or social areas. In order to be eligible for special education services under the category
ASD according to MARSE, determination of eligibility must include ALL three of the following:
(1) Qualitative impairment in reciprocal social interactions
(2) Qualitative impairment in communication
(3) Restricted, repetitive, and stereotyped behaviors
In addition, the student’s disability must have an adverse impact on progress in general education in
academic, social, or behavioral domains that require specialized instruction (i.e. special education).
Results of standardized measures, interviews, and observations are organized within these eligibility
components. Summary of the information represents a preponderance of evidence from all interviews,
surveys, reports, and direct observation and assessments.
NOTE: For information on gathering data for ASD eligibility, review the Education-Based Evaluations
for ASD document published by The Michigan Autism Council.
QUALITATIVE IMPAIRMENT IN RECIPROCAL SOCIAL INTERACTIONS
According to MARSE, to be eligible for special education services under the category of ASD, students
must demonstrate Qualitative Impairment in Reciprocal Social Interactions as evidenced by two of four
of the following eligibility criteria:
• Marked impairments in the use of multiple nonverbal behaviors, such as eye-to-eye gaze, expressions,
body postures, gestures;
• Failure to develop peer relationships appropriate to the student’s developmental level;
• Marked impairment in spontaneous seeking to share enjoyment, interests, or achievements with other
people;
• Marked impairment in the areas of social or emotional reciprocity
Supporting Evidence (e.g. interviews, observations, surveys and standardized scores):
NOTE: Describe all evaluation evidence for or against the presence or absence of a qualitative
impairment in reciprocal social interaction. Include descriptions and explanations of information that
contradicts the conclusion of the presence of absence of this ASD component. When reporting
observation data, indicate the evaluator who specifically observed the examples provided.
QUALITATIVE IMPAIRMENT IN COMMUNICATION
According to MARSE, to be eligible for special education services under the category of ASD, students
must demonstrate Impairment in Communication as evidenced by one of four of the following eligibility
criteria:
• Delay in or absence of spoken language unaccompanied by an attempt to compensate through
alternative modes of communication
The Michigan Autism Council 39 www.michigan.gov/autism
• Marked impairment in pragmatics or the ability to initiate, sustain, or engage in reciprocal
conversations with others
• Stereotyped and repetitive use of language or idiosyncratic language
• Lack of varied, spontaneous, make believe play or social imitative play appropriate to the student’s
developmental level
Supporting Evidence (e.g. interviews, observations, surveys and standardized scores):
NOTE: Describe all evaluation evidence for or against the presence or absence of a qualitative
impairment in communication as it relates to ASD. Include descriptions and explanations of information
that contradicts the conclusion of the presence of absence of this ASD component. When reporting
observation data, indicate the evaluator who specifically observed the examples provided.
RESTRICTED, REPETITIVE, AND STEREOPTYPED BEHAVIORS
According to MARSE, to be eligible for special education services under the category of ASD, students
must demonstrate Restricted, Repetitive and Stereotyped Behaviors as evidenced by one of four of the
following eligibility criteria:
• Encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is
abnormal in intensity or focus
• Apparent inflexible adherence to specific, nonfunctional routines or rituals
• Stereotyped and repetitive motor mannerisms (such as hand flapping or complex whole-body
movements)
• Persistent preoccupation with parts of objects
Supporting Evidence (e.g. interviews, observations, surveys, and standardized scores):
NOTE: Describe all evaluation evidence for or against the presence or absence of restrictive, repetitive,
and stereotyped behaviors as they relate to ASD. Include descriptions and explanations of information
that contradicts the conclusion of the presence of absence of this ASD component. When reporting
observation data, indicate the evaluator who specifically observed the examples provided.
UNUSUAL OR INCONSISTENT RESPONSE TO SENSORY STIMULI
Determination may include unusual or inconsistent response to sensory stimuli:
NOTE: Describe all evaluation evidence for or against the presence or absence of unusual or
inconsistent response to sensory stimuli as it relates to ASD. Include descriptions and explanations of
information that contradicts the conclusion of the presence of absence of this ASD component. When
reporting observation data, indicate the evaluator who specifically observed the examples provided.
DETERMINATION OF OTHER SPECIAL EDUCATION ELIGIBILITY
Should the student be considered eligible under another eligibility category (e.g. Emotionally Impairment
(EI) or Other Health Impairment (OHI), include the eligibility criteria for those conditions and the
relevant supporting evidence in this section.
The Michigan Autism Council 40 www.michigan.gov/autism
SUMMARY RESULTS OF STANDARDIZED MEASURES
Although this information is included in the sections above, a summary of scores is provided here. If the
scores do not support other evidence (e.g. observations, interviews), explain why that might be the case
(e.g. limits in reliability or validity with the MARSE criteria). For information on standardized
assessment considerations, read the Education-Based Evaluations for ASD document published by The
Michigan Autism Council. An example of how to report the summary is provided here:
Example of a summary of direct standardized assessment results:
Autism Diagnostic Observation Schedule (ADOS):
The Autism Diagnostic Observation Schedules (ADOS) is a semi-structured, standardized assessment of
social interactions, communication, play, and imaginative use of materials for children suspected of
having autism. This instrument also provides cut-off points for the broader Autism Spectrum Disorder
diagnosis, including pervasive developmental disorder and atypical autism.
The Communication Domain looks at the following: Amount of Social Overtures/Maintenance of
Attention; Stereotyped / Idiosyncratic Use of Words or Phrases; Conversation; Pointing; Descriptive,
Conventional, Instrumental, or Informational Gestures.
The Reciprocal Social Interaction Domain looks at the following: Unusual Eye Contact; Facial
Expressions Directed to Others; Spontaneous Initiation of Joint Attention; Quality of Social Overtures;
Quality of Social Response; Amount of Reciprocal Social Communication; and Overall Quality of
Rapport.
The ADOS was administered to (student) on (date / time) and resulted in the following scores:
Subscale
Score
Indicative of ASD
Communication Domain
Scores of X or + are indicative of ASD
Reciprocal Social Interaction
Scores of X or + are indicative of ASD
Communication + Social Interaction Domain
Scores of X or + are indicative of ASD
The results of the ADOS are (suggestive or not suggestive) of an Autism Spectrum Disorder and (support
or do not support) the other information gathered and observations conducted.
Example of a summary of rating scale results:
Gilliam Asperger’s Disorder Scale (GADS):
The GADS is a norm-referenced questionnaire designed to aid in the diagnosis of the disorder. The
GADS is made up of four subscales: Social Interaction (e.g. communicative intent and emotional
behaviors), Restricted Patterns of Behavior (e.g. stereotypical and restricted behaviors associated with the
disorder), Cognitive Patterns (e.g. cognitive and language skills), and Pragmatic Skills (e.g. language used
in a social context). Overall results are described as an Asperger’s Disorder Quotient. Quotients above 80
indicate a high / probable likelihood of Asperger’s Disorder (AD).
The GADS was completed by the following individuals resulting in the scores below:
Name of Reporter
Position
AD Quotient
Probability of AD
Special Education Teacher High / Probable
School Social Worker Low / Not Probable
General Education Teacher High / Probable
The Michigan Autism Council 41 www.michigan.gov/autism

Authorized Provider of Speech &
Language Services
Low / Not Probable
Parent High / Probable
SUMMARY AND RECOMMENDATIONS
The goal of a school-based evaluation team for ASD is not to provide a clinical diagnosis of the disorder,
but rather to recommend eligibility and determine the need for special education services. Michigan’s
Special Education definition characterizes ASD by qualitative impairments in reciprocal social
interactions, qualitative impairments in communication, and restricted range of interests or repetitive
behavior. A student must present with deficits in all three domains to meet the requirements for special
education eligibility under the ASD label.
Based on the preponderance of the present observations, survey and interview information, and
standardized measures, the recommendation of the MET is that:
• NOT ELIGIBLE ASD EXAMPLE: The student’s social deficits are more related to
hyperactivity and inattention or behaviors related to difficulties with emotional regulation (i.e.
anxiety and depression) than deficits in the understanding and demonstrating of social reciprocity
as seen in students with ASD. As such, the student a) should be considered eligible under OHI
or EI. NOTE: Ensure that information is provided on these eligibilities in the body of the report
if, in fact, these are considerations in the evaluation, or b) the student is not eligible for special
education.
• ELIGIBLE ASD EXAMPLE: The student is eligible for special education services under ASD.
In addition, the MET would like to offer the IEP team the following recommendations:
NOTE: Include information and recommendations to assist the IEP team in writing the Present Level of
Academic Achievement and Functional Performance (PLAAFP), developing a list of needed
supplemental aids and services, and identifying relevant goals and objectives or benchmarks.
This evaluation team is available for further consultation, if needed.
___________________________________
School Psychologist
___________________________________
School Social Worker
___________________________________
Authorized Provider of Speech and Language Services
Report Compiled by:
The Michigan Autism Council 42 www.michigan.gov/autism
Appendix H
Resources
Michigan Autism Spectrum Disorders State Plan (2012)
www.michigan.gov/documents/autism/ASDStatePlan_2_19_13_Final_414143_7.pdf
Michigan Administrative Rules for Special Education
http://w3.lara.state.mi.us/orrsearch/105_43_AdminCode.pdf
Autism Spectrum Disorder Guideline (Charlevoix-Emmet ISD) (June 2013)
www.charemisd.org/academic/specialeducation/evaluationservices
Wayne County Guidelines for Determining Eligibility and Placement Decisions for
Special Education Under the Autism Spectrum Disorder Rule (2011)
www.resa.net/downloads/special_education_guidelines/autism_guidelines.pdf
Children With Autism Spectrum Disorder: A Guide for Eligibility Determination
Professional Resource Guide (Ottawa Area ISD) (2011)
www.oaisd.org/downloads/_acct_/00/00/01/59/asd_guide_summer_2011_20111207_153626_1.pdf
Oregon Educational Guidelines for ASD
www.livebinders.com/play/play_or_edit?id=168313
Wisconsin Educational Evaluation Guide for Autism (2009)
http://sped.dpi.wi.gov/sites/default/files/imce/sped/pdf/elg-autism-guide.pdf
Autism Internet Modules
www.autisminternetmodules.org
Centers for Disease Control and Prevention Autism Case Training
www.cdc.gov/NCBDDD/actearly/autism
Statewide Autism Resources and Training Centralized Evaluation Team (CET)
www.gvsu.edu/autismcenter/centralized-evaluation-team-cet-96.htm
A Collaborative Approach to ASD Evaluation (2013)
http://maase.pbworks.com/w/file/fetch/68046120/Dunlap%20A%20Collaborative%20Appro
ach%20MSI8-13.pdf
Education-Based Evaluation for ASD
http://maase.pbworks.com/w/file/83431858/12-HQ%20SB%20Evals.Kelly.Dunlap.pdf
Michigan Autism Council Collaboration Matrix (2014)
www.michigan.gov/autism
The Michigan Autism Council 43 www.michigan.gov/autism
References
Durocher, J.S. (2011). Assessment for the purpose of instructional planning for students
with autism spectrum disorders. Autism Spectrum Disorders: Foundations,
Characteristics, and Effective Strategies (Chapter 2). Pearson.
Gilliam, J. (2014). Gilliam Autism Rating Scale, Third Edition (GARS-3). Pro-Ed.
Gilliam, J. (2000). Gilliam Asperger Disorder Scale. PsychoCorp.
Gilliam, J. Klin, A., McPartland, J., & Volkmar, F. R. (2005). Asperger syndrome. Handbook
of autism and pervasive developmental disorders (3rd ed., pp. 88–125). Hoboken, NJ:
Wiley.
Klin, A., Saulnier, C., Tsatsanis, K., & Volkmar, F. R. (2005). Clinical evaluation in autism
spectrum disorders: Psychological assessment within a transdiciplinary framework.
Handbook of autism and pervasive developmental disorders (3rd ed. Vol. 2, pp. 863–
881). Hoboken, NJ: Wiley.
Klin A, Schultz R & Cohen D (2000). Theory of mind in action: developmental perspectives
on social neuroscience. Understanding Other Minds: Perspectives from Developmental
Neuroscience (2nd ed., pp.357–388). Oxford, UK: Oxford University Press.
Krug, D. Arick, J, & Almond, P. (2008). Autism Screening Instrument for Educational
Planning – Third Edition (ASIEP-3). Pro-Ed.
Leventhal-Belfer, L., & Coe, C. (2004). Asperger’s syndrome in young children. London, UK:
Jessica Kingsley Publishers.
Lord, C. & Rutter, M. (2012). Autism Diagnostic Observation Schedule, Second Edition
(ADOS-2). WPS Publishers.
Oates J, & Grayson A. (2004). Cognitive and Language Development in Children. Oxford,
UK: Blackwell Publishing.
Robins, D. Fein, D. & Barton, M. (2009). Modified Checklist for Autism in Toddlers, Revised
with Follow-Up (M-CHAT-R/F). Retrieved from
https://www.m-
chat.org/_references/mchatdotorg.pdf
Rutter, M. & LeCouteur, A. (2003). Autism Diagnostic Interview, Revised (ADI-R). WPS
Publishers.
Schopler, E. & Bourgondien, M. (2010). Childhood Autism Rating Scale, Second Edition
(CARS-2). WPS Publishers.
The Michigan Autism Council 44 www.michigan.gov/autism

Shriver, M.D., Allen, K.D., & Matthews, J.R. (1999). Effective assessment of the shared and
unique characteristics of children with Autism. School Psychology Review, 28, 538-558.
Sikora D.M., Hartley S.L., McCoy R., Gerrard-Morris A. (2008). The Performance of Children
with Mental Health Disorders on the ADOS–G: A Question of Diagnostic Utility. Research
in Autism Spectrum Disorders, 2, 188–197.
Stone, W.L., Lee, E.B., Ashford, L., Brissie, J., Hepburn, S.L., Coonrod, E.E., & Weiss, B.H.
(1999). Can autism be diagnosed accurately in children under 3 years? Journal of Child
Psychology and Psychiatry, 40(2), 219-226.
National Research Council. (2001). Educating children with autism: Committee on
educational interventions for children with autism, division of behavioral and social
sciences and education. Washington, DC: National Academy Press.
The Michigan Autism Council 45 www.michigan.gov/autism
